
Last update: 03/06/2026, Dr. Miguel B. Royo Salvador, Medical Board number 10389. Neurosurgeon and Neurologist.
Definition
Idiopathic scoliosis (I.SCO) consists of a lateral deviation of the spine due to an unknown cause. It is more frequent in females and is mostly observed in the age of growth.

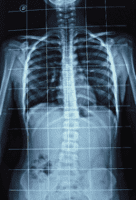
Fig. 5.- Magnetic Nuclear Resonance (MRI) with the coronal section of the spine in case of idiopathic scoliosis. Here, the spinal canal can be seen with the spinal cord going from convexity to convexity inside the vertebral canal, indicating the existence of an important caudal force caused by the cord traction.
Symptoms
Scoliosis’ pathology can be expressed in various clinical symptoms combinations; most frequent in our caseload are: lumbago, thoracic back pain, headaches, gait alterations, back blocks and paraesthesia.
Causes
– According to conventional theories:
Scoliosis is brought about by an imbalance of the paravertebral muscular mass, ligamentous anomaly, proprioceptive postural disorders, the spine’s reaction to forces such as gravity or ligamentous muscle action, inborn error of metabolism, neurological alterations and others.
– According to Filum System® health method:
Idiopathic scoliosis is the result of an avoidance or compensation mechanism of the spine’s reaction to the caudal cord traction, produced by a tense Filum Terminale. This traction force is not evident in the complementary tests such as MRIs.
Other idiopathic spine deviations share the same above-mentioned cause. These idiopathic spine deviations include hyperkyphosis, hyperlordosis, rectification of the spinal curvature, vertebral rotation (Rotoscoliosis) and reversal of the spinal curvatures; sharing the same biomechanical meaning.
Scoliogram / x-ray of the entire spine
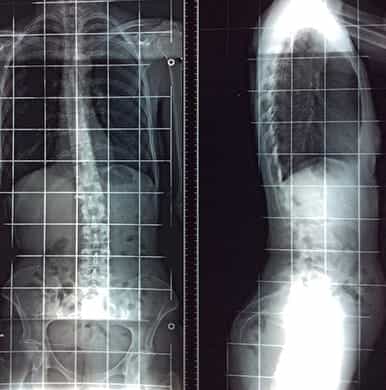
For the diagnosis and follow-up of idiopathic scoliosis, it is essential to view an x-ray of the entire spine, in front and profile views, called Scoliogram.

Front view Scoliogram

Profile view Scoliogram
Other types of Scoliosis: Secondary
Scoliosis can be defined as secondary when the spine has deviated in the frontal or anteroposterior view and this deviation can be attributed to a known cause, such as a tumour, trauma, infection or other.
Risk factors in Idiopathic scoliosis
The risk factors influencing the development of idiopathic scoliosis are the following:
- Family history: the caudal traction produced by the excessively tense Filum terminale, which we define as the Filum Disease, can drive the spine’s deviation mechanism known as Idiopathic Scoliosis. This condition is congenital and can be inherited from one generation to another in a family.
- Age: the beginning of Idiopathic scoliosis is often observed during the period of intense growth of the human body, puberty. It can also be observed in young children or in late adolescence. In this first part of life, the spinal cord traction can increase suddenly, causing the spine deviation.
- Gender: although both boys and girls may suffer from scoliosis, most of the current studies agree that girls are at higher risk of worsening during somatic development.
- Degrees of curvature: regardless of the patient’s age, if the scoliosis curve exceeds 40 degrees then, in standing position, the force of gravity acts additionally to the tractive force originating in a tense Filum Terminale on the curvature. So, when the curvature of the spine is greater than 40-50 degrees of lateral deviation, worsening until reaching levels of serious or severe scoliosis may occur, even of more than 70-90 degrees.
- A sudden increase in spinal cord traction: we have observed that after an accident, fall or trauma to the spine, spinal cord traction may increase when a congenital Filum Disease is present. In these circumstances, the caudal medullary traction is of greater magnitude; hence, worsening of the deviation of the spine can be observed. In these cases, the accident is not the cause of scoliosis, as in the case of trauma-related Scoliosis, but it triggers a worsening of the pre-existing deviation.
Complications from Idiopathic Scoliosis
Depending on the degrees of curvature of the spine deviation, Scoliosis can eventually cause not only collateral damage in the rest of the body but also difficulties and dysfunctions that can increasingly affect the life of the sufferer. Some of the major complications are:
- Chronic pain: Scoliosis can increase the intensity of the back pain, headaches, gait difficulties and the blockages of the back or limbs hence making them chronic.
- Aesthetics: with the development of scoliosis of more than 20-30 degrees, one can start to observe postural and physical changes due to adaptation of the entire organism to the deviation of the spine. These changes alter the patient’s appearance and position, especially by increasing the asymmetry between both body halves. Especially during the phase of adolescence such changes, if they are notorious, can affect the young individual at a psycho-social level apart from affecting at a functional level.
- Thoracic damage: in severe Scoliosis, the rib cage can press on the lungs and the heart, and can hence hinder respiratory and cardiac function.
Treatment of Idiopathic Scoliosis
Since Hippocrates first described Scoliosis as a disease, many attempts have been made to straighten the spine by all possible means; with manipulation, physiotherapy, tractions, braces etc. All these methods were not enough and now surgical straightening of the curved spine is performed by applying metal prostheses.
All treatments are symptomatic and are aimed at correcting the consequence of the disease -the curved spine- since the underlying cause is unknown.
Since 1993, with the publication of Dr Royo-Salvador’s doctoral thesis, a new etiological treatment has been designed which acts on the cause of the disease. This publication relates the caudal traction of the entire nervous system by the Filum Terminale as a cause of idiopathic scoliosis among other diseases. When the Filum Terminale is sectioned surgically according to Filum System® (FS®), the responsible caudal cord traction force is eliminated.
At the Institut Chiari & Siringomielia & Escoliosis de Barcelona, a special health method, the Filum System®, has been designed, which includes the minimally invasive surgical technique to take away the traction force applied by a tense Filum Terminale. This technique has been applied to over 1400 patients and no serious complications have been observed. A subjective change in perception of a spinal release has been observed in all the cases: the bending attitude of Scoliosis disappears in most cases and the spine curvature improves if it is less than 40º. In cases with spine curvatures greater than 40º, we recommend the application of the conventional therapies to mitigate the action of gravity on the spine.
Sectioning Filum Terminale according to the FS®
At Institut Chiari & Siringomielia & Escoliosis de Barcelona, our medical team treats Idiopathic Scoliosis from a neurological and neurosurgical perspective. In this disease, the spinal cord suffers a traction force and hence it is tensed and tight inside the spinal canal. With the application of the Filum System®, the spinal cord traction originating from the tight Filum Terminale is eliminated and the spine curving force of Scoliosis disappears. The simple sectioning of the ligament takes away the traction force on the spinal cord and it stops sending the bending stimulus to the spine, stopping the progression of Scoliosis.
After the Sectioning of the Filum Terminale according to Filum System®, the evolution depends on the degrees of curvature of the spine misalignment. The progression of the Scoliosis curves comes to an halt (for angles 10º- 40º) or can continue progressing (for angles 40º and more) but with slower pace than it would do without the diagnostic criterion and treatments of Filum System®. A decrease in the symptoms and signs is observed in most cases.
In all cases, our medical team will assess the most appropriate post-operative indication for each patient: rehabilitation, corrective muscle stimulation, physiotherapy, braces or spinal fusion.
Results of the Sectioning of the Filum Terminale
At our centre, patients suffering not only from Idiopathic scoliosis as a single disease but also associated with the Arnold-Chiari Syndrome Type I and / or Syringomyelia have been operated. The progression of the disease has stopped and improvements have been obtained. In some case, the results have been spectacular, especially in the cases with curves of than 40 degrees.
– Case no. 17584. Clear decrease in the Scoliosis curve in case of an operated patient – Pre-operative image from 2014 and Post-operative image from 2015.
2014

2015

2009
2011

2012
To learn more, we recommend a visit to the section “Testimonials: Idiopathic scoliosis”. Please note that all published testimonials are for informative purposes only and express the opinions of their authors.
BIBLIOGRAPHY
- Dr. Miguel B. Royo Salvador (1996), Siringomielia, escoliosis y malformación de Arnold-Chiari idiopáticas, etiología común (PDF). REV NEUROL (Barc); 24 (132): 937-959.
- Dr. Miguel B. Royo Salvador (1996), Platibasia, impresión basilar, retroceso odontoideo y kinking del tronco cerebral, etiología común con la siringomielia, escoliosis y malformación de Arnold-Chiari idiopáticas (PDF). REV NEUROL (Barc); 24 (134): 1241-1250
- Dr. Miguel B. Royo Salvador (1997), Nuevo tratamiento quirúrgico para la siringomielia, la escoliosis, la malformación de Arnold-Chiari, el kinking del tronco cerebral, el retroceso odontoideo, la impresión basilar y la platibasia idiopáticas (PDF). REV NEUROL; 25 (140): 523-530
- M. B. Royo-Salvador, J. Solé-Llenas, J. M. Doménech, and R. González-Adrio, (2005) “Results of the section of the filum terminale in 20 patients with syringomyelia, scoliosis and Chiari malformation“.(PDF). Acta Neurochir (Wien) 147: 515–523.
- M. B. Royo-Salvador (1992), “Aportación a la etiología de la siringomielia“, Tesis doctoral (PDF). Universidad Autónoma de Barcelona.
- M. B. Royo-Salvador (2014), “Filum System® Bibliography” (PDF).
- M. B. Royo-Salvador (2014), “Filum System® A brief guide”.