
Last update: 03/20/2026, Dr. Miguel B. Royo Salvador, Medical Board number 10389. Neurosurgeon y Neurologist.
Definition
In normal conditions, the spinal cord is held within the spinal canal only by the denticulate ligaments and the filum terminale, a ligament that connects the conus medullaris to the first coccygeal vertebrae.
When the mobility of the spinal cord within the bony spinal canal is limited by the presence of a non-visible spina bifida that produces a tethering, the clinical picture is defined as Tethered Cord Syndrome.
The Tethered Cord Syndrome can be congenital or acquired.
The Tethered Cord Syndrome with occult spina bifida or “Occult Tethered Cord Syndrome” ” is congenital.
Occult tethered cord or “Occult Tethered Cord Syndrome” is associated with an occult spina bifida. This is a neuro-spinal malformation that is characterized by the incomplete development of the spinal cord (predominantly in the lumbar region) which is anchored by the malformation, producing mechanical injuries due to the traction, mainly in the spinal cord and spine (Fig.1).
A spina bifida is defined as occult when it is not visible externally. This is the most common and mildest type of spina bifida, that produces a small separation or gap in one or more vertebrae of the spine. Sometimes it is possible to observe visible signs on the newborn’s skin above the spinal defect, such as a birthmark, an abnormal tuft of hair or a dimple.
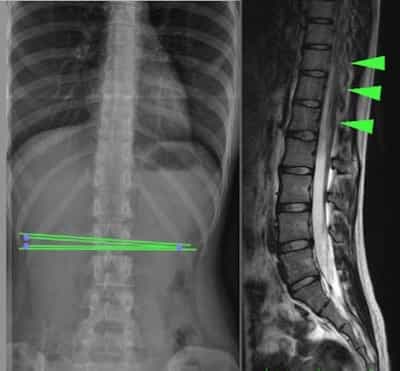
Fig.1
Diagnosis
The clinical picture of a tethered cord with occult spina bifida can be determined at birth, although in most patients the neurological symptoms and signs develop in the first two decades of their life, mainly during adolescence, hence the diagnosis is usually made in adulthood. Many patients actually discover the condition through tests done for unrelated reasons.
To detect and diagnose it, it is necessary to perform complementary tests like a Nuclear Magnetic Resonance (MR) or a Computerized Axial Tomography (CT) or a simple X-ray of the spine level where the tethering is located.
Symptoms
As the spinal nerves are usually not involved in a tethered cord with occult spina bifida, there may be no manifest sign or symptom in the whole patient’s life, or they can remain mild for many years.
Apart from the mentioned skin marks, in most cases symptoms mainly consist of: sensitivity and motor disorders in the lower extremities, with weakness that can cause gait difficulties, sphincter alterations – such as neurogenic bladder – that manifests with enuresis or repeated urinary infections, and pain-related symptoms especially in the lumbar spine, sciatica, etc.
Once the neurological symptoms appear, most of them are irreversible. Therefore, these conditions need an early diagnosis, in order to prevent them through treatment.
Causes
The causes of occult spina bifida and, consequently, of the associated tethered cord, are the result of a combination of genetic predisposition, environmental factors and family history. They can be related to neural tube defects and folate deficiency.
In general, the neural tube forms in the early stages of pregnancy and closes by day 28 after conception. In babies with spina bifida, both mild and occult, part of the neural tube does not form or close properly, producing defects in the development of the spinal cord and vertebral column. This malformation is usually associated with the presence of low levels of folic acid during pregnancy.
Risk Factors
Some factors are associated with an increased risk of occult spina bifida:
- Female gender: women are more affected than men.
- Family history: predisposition to occult tethered cord depends on a genetic susceptibility, especially related to neural tube defects.
- Folate deficiency and of other metabolic and environmental agents: these are additional factors that can contribute to the development of neural tube defects during pregnancy.
Complications
The first complication in an occult spina bifida is the same tethered cord that it causes, with its early and progressive development.
The complications that can be observed in patients with occult tethered cord include:
- A slow and progressive sphincter neurological deterioration, with an in crescendo weakness of the lower extremities.
- Increase in pain, especially at lumbar level, and in the sensitivity affectation of lower extremities, with the consequent worsening of the patient’s quality of life.
- Spinal cord lesions and associated injuries: the irreversibility of some symptoms, caused and aggravated by the occult tethered cord, can lead to several associated urological and orthopaedic diagnoses.
Treatment
The treatment for occult Tethered cord is exclusively neurosurgical: once the level of the tethering is detected, the most adequate surgical method is applied in order to remove any cord adherence.
When to operate, with which technique and at what level will depend on each specific case and on the criteria the surgeon will apply with each patient. Some surgeons prefer to wait for the patient to present symptoms or even to reach an advanced stage of the condition, while others operate to prevent neurological symptoms from appearing, as they can be irreversible.
Outcomes
Our centre is highly specialized in a diagnosis that is often confused with an occult tethered cord – the Filum Disease.
The Filum System® method, that we apply at the Institut Chiari & Siringomielia & Escoliosis de Barcelona, includes not only a refined and minimally invasive technique for cases with Filum Disease, but also other techniques for the release of an occult tethered cord, which imply a different surgery for each specific case. We personalize and apply the least invasive and most adequate and efficient detethering neurosurgical method for each patient.
At our centre we obtained excellent results in most operated cases, with a minimum number of complications, null mortality and neurological complications rate out of a total 83 surgical procedures.
Bibliography
- J1. Guerra LA, Pike J, Milks J, Barrowman N, Leonard M. Outcome in patients who underwent tethered cord release for occult spinal dysraphism. J Urol. 2006 Oct;176 (4 Pt 2):1729-32.
- 2. Hoffman HJ, Hendrick EB, Humphreys RP. “The Tethered Spinal Cord: its protean manifestations, diagnosis and surgical correction”. Childs Brain. 1976;2(3):145-55.
- Dr. Miguel B. Royo Salvador (1996), Siringomielia, escoliosis y malformación de Arnold-Chiari idiopáticas, etiología común (PDF). REV NEUROL (Barc); 24 (132): 937-959.
- Dr. Miguel B. Royo Salvador (1996), Platibasia, impresión basilar, retroceso odontoideo y kinking del tronco cerebral, etiología común con la siringomielia, escoliosis y malformación de Arnold-Chiari idiopáticas (PDF). REV NEUROL (Barc); 24 (134): 1241-1250
- Dr. Miguel B. Royo Salvador (1997), Nuevo tratamiento quirúrgico para la siringomielia, la escoliosis, la malformación de Arnold-Chiari, el kinking del tronco cerebral, el retroceso odontoideo, la impresión basilar y la platibasia idiopáticas (PDF). REV NEUROL; 25 (140): 523-530
- M. B. Royo-Salvador, J. Solé-Llenas, J. M. Doménech, and R. González-Adrio, (2005) “Results of the section of the filum terminale in 20 patients with syringomyelia, scoliosis and Chiari malformation“.(PDF). Acta Neurochir (Wien) 147: 515–523.
- M. B. Royo-Salvador (2014), “Filum System® Bibliography” (PDF).
- M. B. Royo-Salvador (2014), “Filum System® Guía Breve”.
Understand the difference among the diagnoses of Occult tethered cord syndrome, Tethered cord syndrome y Filum Disease