
Last update: 03/20/2026, Dr. Miguel B. Royo Salvador, Medical Board number 10389. Neurosurgeon y Neurologist.
Definition
Brainstem Kinking (BSK) or Brainstem Angulation consists in a forward projected angle of the brainstem, formed between the pons and the spinal cord. These structures (pons and medulla) tend to form an angle at the bulbomedullary level. A discrete angulation is found quite frequently on normal imaging studies. A very pronounced angulation is however not frequent.
It tends to be accompanied by Platybasia, Basilar Invagination and Odontoid retroflexion, especially in very pronounced cases. It is also frequently associated with the Arnold-Chiari Syndrome Type I.
It is studied as an independent malformation, as it may or may not represent the morphological repercussion on the nervous system of the aforementioned craniocervical malformations.
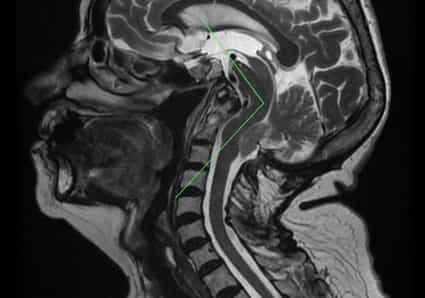
Fig.1.- Sagittal craniocervical MR image with Brainstem Kinking at the level of the pons and the medulla oblongata – spinal cord. Furthermore, there is Basilar Invagination, Odontoid retroflexion and a descent of the cerebellar tonsils. The increase of the supracerebellar space should be pointed out as it is supporting evidence for the traction theory and contradictory of the theory of a malformation with a small posterior fossa.
Symptoms
Brainstem angulation is diagnosed through imaging (MRI or CT) and is not inherently accompanied by symptoms, unless it manifests together with clinical picture of the other frequently associated skull malformations.
Nuclear Magnetic Resonance
The diagnosis and monitoring of Brainstem Angulation is carried out through imaging, with a Nuclear Magnetic Resonance (NMR), namely a brain or skull NMR (see Fig.1).
Causes
– According to conventional theories:
Brainstem Kinking is associated to several possible congenital causes, for example alpha-dystroglycanopathies.
– According to the health method Filum System®:
According to Dr. Royo-Salvador’s theory, the observed brainstem kinking is due to a congenital mechanism of growth asynchrony between spinal cord and central nervous system and the spine in the embryonic phase. This produces an abnormal cord traction force that is transmitted by the filum terminale from the coccyx up to the skull, spinal cord and brain. The bony skull deformation together with that of the encephalon determine the form and intensity of the nervous tissue angulation. The more important the bony malformations, determined by the traction, are, the more prominent will be the deformation of the kinked brain stem.
Brainstem Kinking shares the cause of the excessive traction produced by an overly tense Filum Terminale with the Arnold-Chiari Syndrome Type I, idiopathic Syringomyelia and idiopathic Scoliosis, as well as other associated malformations of the craniocervical junction (they are all different manifestations of the Filum Disease).
Risk factors
The most influential risk factor in the development of Brainstem Kinking is the family history: as a congenital condition, it can be inherited between family members. And it shares genetic incidence with the Filum Disease. The disease mechanism of which can be found in all human embryos, and its translation into clinical manifestations depends on the intensity, context and form of expression of this mechanical conflict.
Complications
The complications of Brainstem Angulation can depend on the degree of caudal traction and the resulting mechanical conflict in the foramen magnum. The latter conditions the magnitude, intensity or degree of the conflict between the traction of the spinal cord and the brain stem.
- Sudden death: can occur due to injuries of the nuclei concerned with cardiorespiratory functions in the brainstem where the mechanical conflict takes place. Respiratory disorders during sleep can constitute an aspect of the condition, finding expression in apnoea, respiratory failure or even in the form of sudden death. Hence the importance of an early diagnosis and treatment.
Treatment
Currently, the craniectomy or suboccipital decompression is the standard treatment performed in most centres worldwide for this diagnosis. This surgical practice causes more morbidity and mortality than the natural evolution of the condition itself.
Since 1993, however, with the publication of Dr Royo-Salvador’s doctoral thesis, which links the caudal traction of the entire nervous system due to the filum terminale to being the cause of Brainstem Kinking – among other diseases -, a new treatment has been designed. It is in this case etiological (cause-related) since the caudal cord traction force responsible for the pathological mechanism is eliminated by surgically sectioning the filum terminale.
The sectioning of the filum terminale eliminates tension in the area of the mechanical conflict and alleviates the neurological injuries. The deformations remain for the most part, the traumatic injuries on the other hand are halted thanks to the release of the traction on the entire nervous system, and especially in the area of the angulation.
Our technique for the sectioning of the Filum terminale (SFT) is minimally invasive and it usually indicated as soon as possible in all cases, from mildly to severely symptomatic, as its risks are minimal, much lower than those of the condition itself, and it also stops the condition’s progression.
Suboccipital Craniectomy:
(Foramen magnum decompression)
Outcomes of the Sectioning of the Filum Terminale
More than 1500 Arnold-Chiari I patients, with or without idiopathic Syringomyelia and/or idiopathic Scoliosis, have already undergone surgery according to the Filum System® method.
The purpose of the surgical procedure is to eliminate the cause in order to halt the evolution of the disease and of the mechanical conflict – in the case of brainstem kinking especially of the associated neurological manifestations – and that the patient’s quality of life does not deteriorate.
References
- Royo-Salvador, M.B.; Fiallos-Rivera, M.V.; Salca, H.C.; Ollé-Fortuny, G. (2020), The Filum disease and the Neuro-Craniovertebral syndrome: definition, clinical picture and imaging features, 20:175, BMC Neurology
- Royo-Salvador M.B. (1996), Platibasia, impresión basilar, retroceso odontoideo y kinking del tronco cerebral, etiología común con la siringomielia, escoliosis y malformación de Arnold-Chiari idiopáticas (PDF). REV NEUROL (Barc); 24 (134): 1241-1250
- Royo-Salvador M.B. (1997), Nuevo tratamiento quirúrgico para la siringomielia, la escoliosis, la malformación de Arnold-Chiari, el kinking del tronco cerebral, el retroceso odontoideo, la impresión basilar y la platibasia idiopáticas (PDF). REV NEUROL; 25 (140): 523-530
- Royo-Salvador M.B., Solé-Llenas J., Doménech J.M., González-Adrio R. (2005) “Results of the section of the filum terminale in 20 patients with syringomyelia, scoliosis and Chiari malformation“.(PDF). Acta Neurochir (Wien) 147: 515–523.
Filum Disease
Dr. Royo-Salvador, with his research and doctoral thesis (1992), proved the theory that considers several diseases of unknown cause (such as brain stem kinking, basilar invagination, Arnold-Chiari Syndrome Type I, idiopathic Syringomyelia, idiopathic Scoliosis, platybasia, odontoid retroflexion, and others) as part of a new disease concept (the Filum Disease) and that they share a common cause (spinal cord and entire nervous system traction). When the mechanical conflicto is not of congenital origin, the name is Neuro-cranio-vertebral syndrome.
The mechanical conflicto that determines the traction force of the entire nervous system in the Filum Disease occurs in all human embryos, hence they all suffer its consequences to a greater or lesser extent, and the consequences manifest in many different ways and intensities.
Other diseases, such as herniated discs, some cerebral vascular insufficiency syndromes, facet joint and Baastrup syndromes, fibromyalgia, chronic fatigue, nocturnal enuresis, urinary incontinence and parapareses, are related, due to their cause, to the Filum Disease.
A health method, the Filum System®, has been designed to specify the diagnosis, provide guidance for the treatment and follow-up of the Filum Disease.