Last update: 03/19/2026, Dr. Miguel B. Royo Salvador, Medical License Number 10389. Neurosurgeon and Neurologist.
Definition
Arnold-Chiari I syndrome consists of herniation of the lower part of the brain – the cerebellar tonsils – and the lower cerebellum through the occipital foramen into the vertebral canal, without other associated spinal cord malformations. For some, the descent of the cerebellar tonsils must be greater than 5 mm, for others 3 mm, and for some it may be 0 mm, or impacted tonsils with a compatible clinical picture.

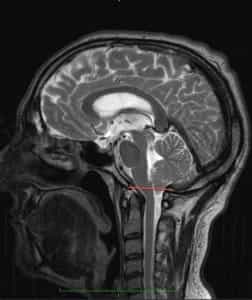
Figure 1.- Diagram showing cerebellar tonsil descent and the consequent increase in the supracerebellar space as the entire cerebellum shifts toward the vertebral canal in Arnold-Chiari I syndrome.
Symptoms
The clinical presentation of Arnold-Chiari I syndrome (ACIS) can manifest in various combinations of symptoms, the most frequent in our case series being (from most to least common): headache, neck pain, limb paresis, vision impairment, limb pain, paresthesia, sensory alteration, vertigo, swallowing difficulty, low back pain, memory impairment, altered gait, upper back pain, balance disturbance, dysesthesia, speech disorder, sphincter alteration, insomnia, vomiting, loss of consciousness, tremor.
Types of Arnold-Chiari Syndrome

There are four classic types (I, II, III, IV) and two recently described types (“0”, “1.5”):
Type I. Descent of the cerebellar tonsils without other central nervous system (CNS) malformations.
Type II. Descent of the cerebellar tonsils with neurovertebral malformation, which may fix the spinal cord to the vertebral canal.
Type III. Descent of the cerebellar tonsils with occipital encephalocele and cerebral abnormalities.
Type IV. Descent of the cerebellar tonsils with cerebellar aplasia or hypoplasia associated with aplasia of the tentorium cerebelli.
Type “0”. Cases have been reported with the clinical features of ACIS but without cerebellar tonsil descent.
Type “1.5”. Recently described, Arnold-Chiari “1.5” syndrome involves cerebellar tonsil descent and brainstem herniation into the occipital foramen.
Causes of Cerebellar Tonsil Descent: Theories
Cerebellar tonsil descent (CTD) may result from traction exerted on the spinal cord by malformations associated with certain forms of Arnold-Chiari syndrome; except in Type I, where tonsil descent is the only morphological alteration – in this case, several theories exist:
– Conventional theories:
- Hydrodynamic: Tonsil descent results from cerebrospinal fluid (CSF) circulation anomalies.
- Malformative: The small cranial fossa theory suggests that this malformation induces the cerebellum to herniate into the vertebral canal.
– Spinal traction theory according to the Filum System ®:
Dr. Miguel B. Royo Salvador’s theory considers cerebellar tonsil descent in Arnold-Chiari I syndrome as the result of abnormal spinal cord traction caused by an anomalous and excessively tense filum terminale ligament (not detectable on complementary examinations).
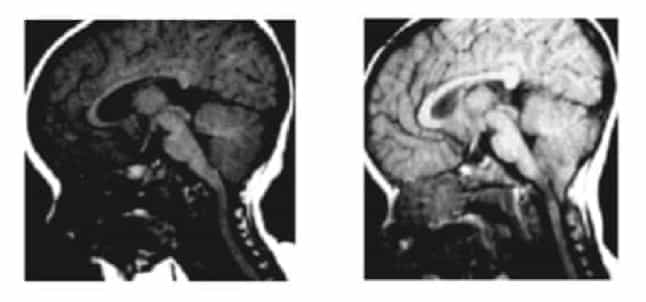
Figure 2.- MRI of a patient at 8 and 20 months, showing CTD developing between the two scans. Huang P. “Acquired” Chiari I malformation. J. Neurosurg 1994. Indicating that besides a genetic/hereditary component, an acquired factor exists.
Risk Factors for Arnold-Chiari I Syndrome
The main risk factors influencing Arnold-Chiari I syndrome development are:
- Family history: Caudal traction of the entire nervous system caused by an excessively tense filum terminale, defined as Filum Disease, responsible for cerebellar tonsil descent. This is a congenital pathology that may be inherited.
- Sudden increase in spinal traction: Following an accident, fall, or spinal trauma in patients with congenital Filum Disease, spinal traction may increase. This may worsen cerebellar tonsil descent or foramen magnum compression symptoms. The accident does not cause tonsil descent but triggers sudden worsening of the preexisting traction mechanism, both anatomically and clinically.
Complications of Arnold-Chiari I Syndrome
Complications from cerebellar tonsil ectopia depend on the degree of caudal traction or compression at the occipital foramen, determined by the conflict between spinal cord and brainstem traction and the available space in the foramen.
- Worsening quality of life: Headaches, vertigo, spinal or limb pain, paresis, swallowing or sensory alterations, cognitive and visual disturbances, or gait changes may become chronic, intensifying over time and limiting normal activity.
- Chronic pain: Patients may require pain unit treatment, as first-line anti-inflammatory or analgesic medications may be insufficient for headache crises and pain symptoms.
- Sudden death: Due to brainstem control of cardiorespiratory functions where cerebellar tonsils exert compression, sleep-related respiratory disorders may occur, including apnea, respiratory failure, or sudden death. Early diagnosis and treatment are critical.
Treatments for Arnold-Chiari I Syndrome
The conventionally accepted treatment for Arnold-Chiari I syndrome is neurosurgical.
Currently, suboccipital craniectomy or decompression is the standard treatment performed worldwide for this diagnosis, with or without syringomyelia, especially in symptomatic cases, as it carries more morbidity and mortality than the natural evolution of the disease.
Since 1993, following Dr. Royo Salvador’s doctoral thesis linking caudal traction of the nervous system via the filum terminale as a cause of cerebellar tonsil ectopia and other diseases, a new etiological treatment has been designed: surgical section of the filum terminale to eliminate the caudal traction responsible for the pathology.
Our Filum Terminale Section (FTS) technique is minimally invasive and is indicated in all cases, symptomatic or asymptomatic, as early as possible, with minimal risks far below those of the disease itself, while halting its progression.
Suboccipital craniectomy:
(Foramen magnum or occipital hole decompression)

Due to the complications and mortality of suboccipital craniectomy, higher than the spontaneous course of Arnold-Chiari I syndrome, we consider it contraindicated.
Results of Filum Terminale Section
Using the Filum System® method, over 1,500 patients with Arnold-Chiari I syndrome, with or without idiopathic syringomyelia and/or idiopathic scoliosis, have been operated on.
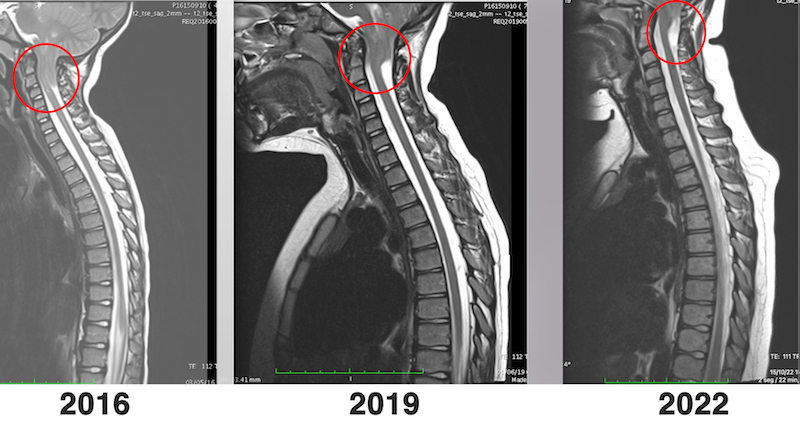
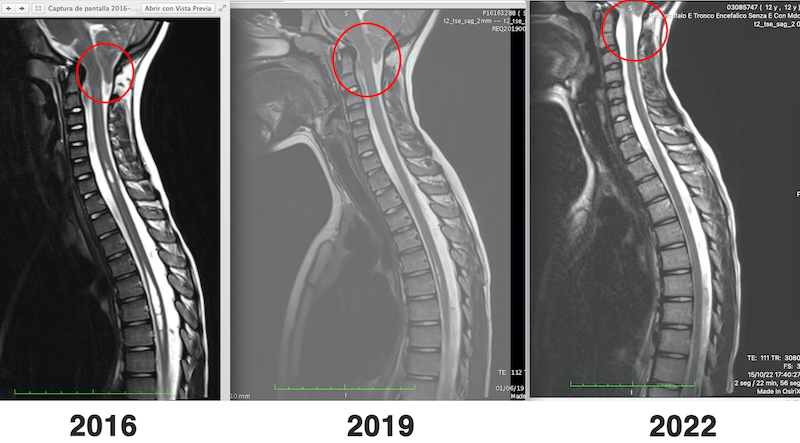
The goal of surgery is to halt disease progression and prevent further ectopia or lesions. However, in some cases, significant clinical improvements have been achieved, even with ascent of the cerebellar tonsils.
Examples: