Last update: 14/03/2025, Dr. Miguel B. Royo Salvador, Medical Board number 10389. Neurosurgeon y Neurologist.
Ehlers-Danlos syndrome (EDS) is a complex group of heterogeneous inherited disorders characterised by fragility of soft connective tissues, joint hypermobility, skin extensibility, vascular complications.
Its clinical manifestation can vary significantly, including several different types: classical EDS, hypermobile EDS, dermatosparaxis EDS, musculocontractural EDS, vascular EDS, arthrochalasia EDS, cardiac-valvular EDS, periodontal EDS, spondylodysplastic EDS, X-linked EDS, brittle cornea syndrome, classical-like EDS type 1 and type 2, kyphoscoliotic EDS and myopathic EDS.
The clinical picture includes a wide variety of symptoms depending on the type of EDS:
In general, in Ehlers-Danlos syndromes, there are genetic mutations that influence the production of collagen and, in some subtypes, of other proteins that interact with it.
This causes the connective tissue to weaken.
Depending on how an organ or tissue is affected, that will cause one type of EDS or another.
According to the Filum System® (FS®), the vertebral disease in EDS can be due to a possible Neuro-cranio-vertebral syndrome (NCVS), a consequence of the spine elongation produced by the laxity of its components and the traction of the Central Nervous System (CNS) and especially of the spinal cord.
The diagnosis is generally based on the patient’s anamnesis and family history, being this condition hereditary. Afterwards, it addresses the type of EDS based on clinical criteria.
A second diagnostic stage involves genetic testing, that is inconclusive but can be exhaustive based on the suspected type of EDS.
According to the FS®, the diagnosis of NCVS associated to EDS is carried out through a clinical examination and complementary testing, such as MRIs of the brain and spine and a full spine x-ray (Scoliogramme).
Family history can be a risk factor in some cases.
Generally, life expectancy is normal, although in certain types of EDS, potentially severe complications may occur.
Joint dislocations and early-onset arthritis can occur.
Fragile skin may develop prominent scarring, or surgical sutures can tear the fragile tissue and make the wound healing difficult.
People with vascular EDS are at risk of suffering potentially fatal ruptures of major blood vessels.
Some organs, such as the uterus and intestines, can rupture as well. Pregnancy can increase the risk of rupture of the uterus and the fragility of maternal tissues may complicate episiotomy or caesarean section. Prenatal, perinatal and postnatal haemorrhage can occur.
Surgical complications may occur due to the fragility of deep tissues.
Mild synovial effusions, sprains and dislocations are common.
Other potentially severe complications are arteriovenous fistulas, visceral ruptures and pneumothorax or hemopneumothorax.
According to the Filum System®:
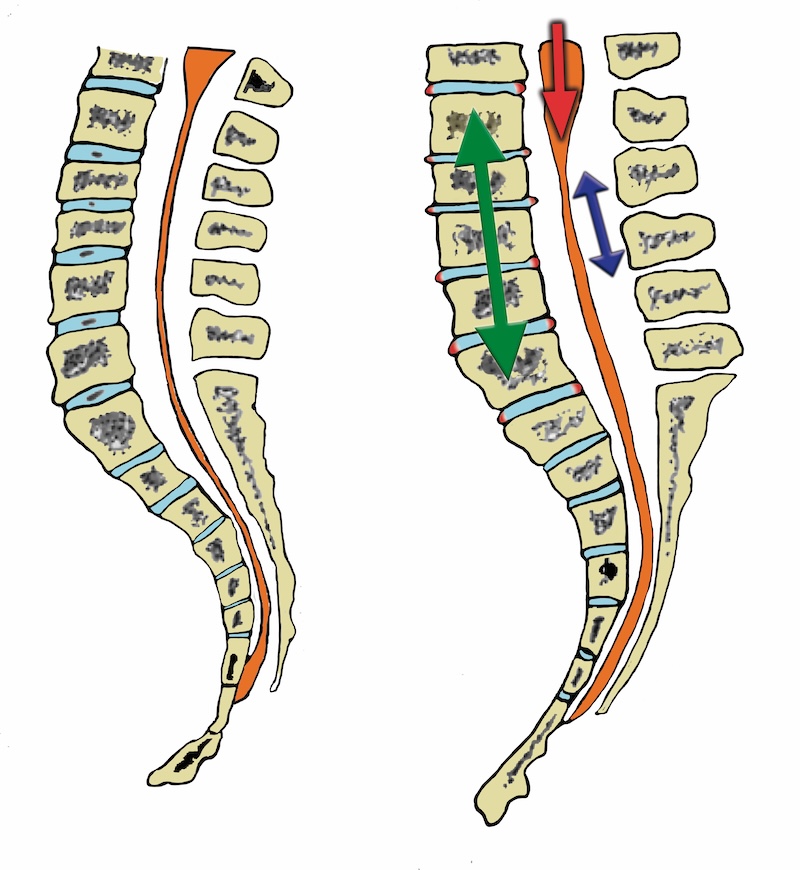
The NCVS associated to EDS is the result of the vertebral elongation and consequent traction of the CNS with the spinal cord, Figure 1.
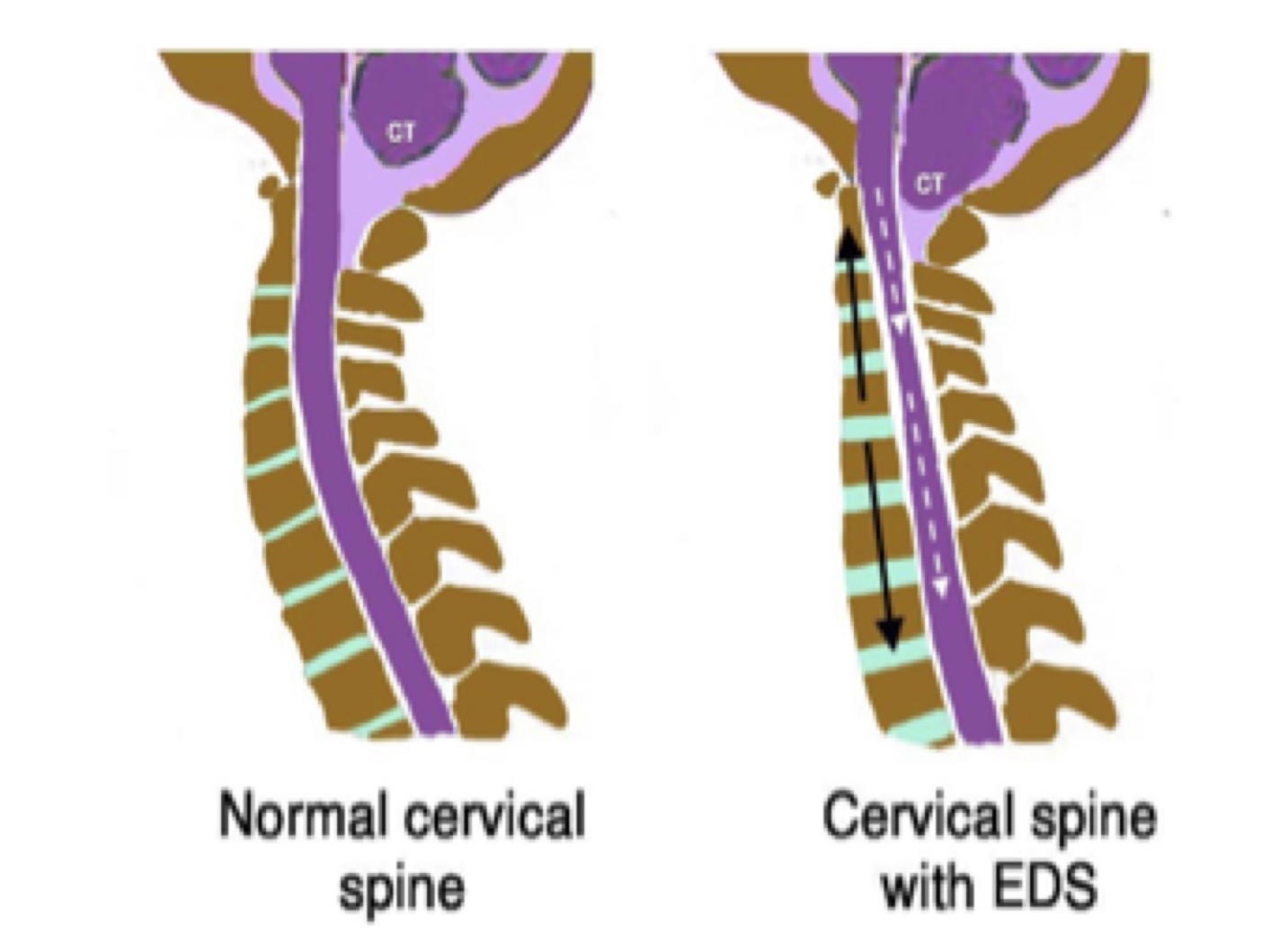
In recent histological studies, the Filum terminale in EDS is paradoxically observed to be more rigid and inelastic than normal (Klinge 2022). According to the FS® criteria, the Filum Terminale in EDS could loose elasticity – even the one that is increased by EDS – due to the constant traction produced by the elongation of the spine, Figure 2.
According to current alarmist criteria, patients with EDS may experience spinal neurological complications, including cervicomedullary symptoms resulting from craniocervical or cervical instability/hypermobility, as well as tethered cord and occult tethered cord syndrome.
However, a review of the literature shows that there are no relevant severe cases that justify that.
On the other hand, at ICSEB we have a series of patients with Ehlers-Danlos Syndrome compatible with Neuro-cranio-vertebral Syndrome and Filum Disease.
For this reason, based on our studies on this topic, we consider that the symptomatology that other authors attribute to craniocervical and/or atlantoaxial instability in cases with EDS cannot be related to this mechanism. It probably reflects an undiagnosed Neuro-cranio-vertebral Syndrome.
For Ehlers-Danlos syndrome, the usual treatment is conservative and symptomatic,
– since currently there is no effective treatment for the connective tissue – and involves
pain management, blood pressure management and physical therapy for muscle strength and joint stability.
Surgery to repair joints damaged by repeated dislocations or to repair lesions in blood vessels and organs. Surgical procedures are also carried out in cases of joint subluxations, such as joint stabilisation and specific nerve release procedures that can provide symptomatic relief when conservative measures fail.
In current clinical practice, there is a significant tendency to consider EDS to be a frequent cause of cervical vertebral dislocation, with the consequent neurological and and vital risk. Therefore, surgical treatments for the arthrodesic consolidation of the cervical spine are indicated with a large deployment of osteosynthesis. According to bibliographic case studies, these treatments are not justified.
According to the Filum System®
Given the evidence obtained from our case series when observing multiple craniovertebral or neurological manifestations in patients with Ehlers-Danlos syndrome, in these cases it is advisable to proceed with a search for clinical and imaging characteristics suggestive of abnormal caudal traction, Neuro-cranio-vertebral syndrome, as well as tests that will help demonstrate craniocervical instability.
Once the association of EDS with the diagnosis of Neuro-cranio-vertebral syndrome is confirmed, the indication of the sectioning of the Filum terminale according to the FS® must be assessed as a treatment.
The results of the sectioning of the Filum terminale surgery in these patients are apparently comparable to those of the main group of surgical patients affected by Neuro-cranio-vertebral syndrome.
With appropriate diagnosis and treatment according to the FS®, the outcomes are comparable to those obtained in the Filum Disease and Neuro-cranio-vertebral syndrome due to other causes.
Monday to Thursday: 9-18h (UTC +1)
Friday: 9-15h (UTC +1)
Saturday and Sunday closed
Toll-free from the US: +18882012544
+34 932 800 836
+34 932 066 406
Legal regulations
Legal notice
Pº Manuel Girona, nº 32
Barcelona, España, CP 08034

The Institut Chiari & Siringomielia & Escoliosis de Barcelona (ICSEB) complies with the established in EU regulation 2016/679 (GDPR).
The contents of this website are a non-official translation of the original content of the website in Spanish. The translation is courtesy of the Institut Chiari & Siringomielia & Escoliosis de Barcelona with the purpose of facilitating comprehension for anyone who wishes to Access the website.