Last update: 09/03/2023, Dr. Miguel B. Royo Salvador, Medical Board number 10389. Neurosurgeon y Neurologist.
Odontoid Retroflexion (OR) is a malformation of the upper portion of the cervical spine consisting of a backward tilting of the odontoid process, displacing and compressing the adjacent nerve structures.
It consists of an invagination of the tip of the odontoid process which is abnormally directed backwards, clearly exceeding the imaginary line between the posterior clinoid processes and the postero-inferior angle of the C2 vertebral body.
OR is often associated with Platybasia and Basilar Impression, and sometimes its presence and size does not match the others.
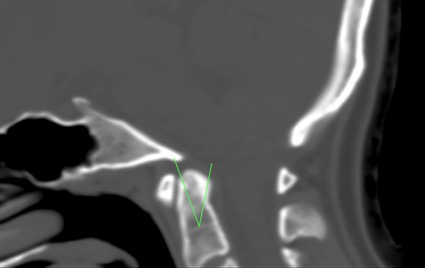
Fig.1 Odontoid Retroflexion. Craniocervical CT.
The symptoms of Odontoid Retroflexion are part of the Basilar Impression and Platybasia picture, the result of compression of the odontoid process on the brain stem and the immediate vascular structures.
The neurological manifestations are typical of a compression of the upper cervical spinal cord: cervical pain, contractures, loss of strength, spasticity, paresis, gait instability, dysmetria and progressive loss of sensation. It may be involved in a chronic increase in intracranial pressure.
Diagnosis of odontoid retroflexion is radiological, and can be made by CT scan (Fig.1) or MRI (Fig. 2) of the skull or brain and cervical spine or cervical spinal cord.
The diagnosis can be assessed by tracing the Thiébaut-Wackenheim-Vrousos basal line, which is a downward extension of the basal plane, and the odontoid process of the axis is usually tangential, or it is no more than two millimeters away from this line.
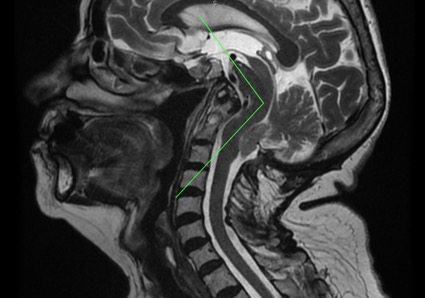
Fig.2.- Sagittal craniocervical MRI showing odontoid retroflexion. Also: basilar impression, descent of the cerebellar tonsils, brainstem kinking. Note the enlargement of the supracerebellar space, evidence for the traction theory and against the theory of the malformation being due to a narrowing of the posterior fossa.
– According to traditional theories:
Like all anomalies of the cranio-cervical junction, odontoid retroflexion is conventionally attributed to congenital – structural or general/systemic issues – or acquired alterations.
– According to the Filum System ® health method:
The deformity found in odontoid retroflexion is due to a congenital mechanism of asynchrony in growth, in the embryonic phase, between the spinal cord and the central nervous system with the spinal column. This generates an anomalous spinal traction force that is transmitted from the coccyx to the axis (C2) and skull, via the filum terminale. The more intense and earlier this traction is applied, the greater the relevance of the bony manifestations such as odontoid retroflexion.
OR shares the cause of caudal traction produced by an excessively tense filum terminale with the Arnold-Chari Syndrome type I, idiopathic Syringomyelia and idiopathic scoliosis, as well as with other associated malformations of the occipital junction. They are all different manifestations of Filum Disease. The earlier and more intense the onset of caudal traction coinciding with osteogenesis, the greater the bony manifestation such as Odontoid retroflexion, basilar impression and platybasia.
In terms of risk factors, family history plays the most significant role in odontoid retroflexion: it is a congenital condition that can be passed down from one relative to the next. In addition, it shares the same genetic incidence as Filum disease. This pathological mechanism is found in all human embryos, but its clinical translation depends on the intensity, environment, and form of expression of this mechanical conflict.
In OR, complications may result from the degree of caudal traction or mechanical conflict within the foramen magnum. The latter determines the extent and intensity or degree of conflict between spinal cord traction and brainstem.
The conventionally accepted treatment for OR is neurosurgical.
Currently, craniectomy or suboccipital decompression is the standard treatment performed in most centres worldwide for this diagnosis. It is usually indicated mainly in symptomatic cases, as it causes more morbidity and mortality than the natural evolution of the pathology itself.
However, since the publication of Dr. Royo-Salvador’s doctoral thesis in 1993, in which the caudal traction of the entire nervous system by the filum terminale is described as the cause of cerebellar tonsillar ectopia -among other conditions- a new treatment has been developed. This treatment is aetiological, since surgically sectioning the filum terminale eliminates the caudal medullary traction force responsible for the pathological mechanism.
Our technique of sectioning the filum terminale (SFT) is minimally invasive and usually indicated in all cases, symptomatic or not, as soon as possible, since it carries minimal risks, much less than those of the pathology itself, and also stops its progression.
More than 1500 patients have already undergone surgery according to the Filum System® method.
The purpose of the intervention is to eliminate the cause, the mechanical conflict between the deformation and the caudal traction of the entire central nervous system and thus to stop the evolution of the disease, especially the associated neurological manifestations in the case of OR, so that the patient’s quality of life does not deteriorate further.
Dr. Royo-Salvador, with his research and doctoral thesis (1992), proved the theory that considers several diseases of unknown cause (Arnold-Chiari Syndrome Type I, idiopathic Syringomyelia, idiopathic Scoliosis, platybasia, basilar invagination, odontoid retroflexion, brain stem kinking, and others) as part of a new disease concept (the Filum Disease) and that they share a common cause (spinal cord and entire nervous system traction).
The traction force of the entire nervous system in the Filum Disease occurs in all human embryos, hence they all suffer its consequences to a greater or lesser extent, and the consequences manifest in many different ways and intensities.
Other diseases, such as herniated discs, some cerebral vascular insufficiency syndromes, facet joint and Baastrup syndromes, fibromyalgia, chronic fatigue, nocturnal enuresis, urinary incontinence and pronounced paraparesis, are related, due to their cause, to the Filum Disease.
A health method, the Filum System®, has been designed to specify the diagnosis, provide guidance for the treatment and follow-up of: Filum System®.
Monday to Thursday: 9-18h (UTC +1)
Friday: 9-15h (UTC +1)
Saturday and Sunday closed
Toll-free from the US: +18882012544
+34 932 800 836
+34 932 066 406
Legal regulations
Legal notice
Pº Manuel Girona, nº 32
Barcelona, España, CP 08034

The Institut Chiari & Siringomielia & Escoliosis de Barcelona (ICSEB) complies with the established in EU regulation 2016/679 (GDPR).
The contents of this website are a non-official translation of the original content of the website in Spanish. The translation is courtesy of the Institut Chiari & Siringomielia & Escoliosis de Barcelona with the purpose of facilitating comprehension for anyone who wishes to Access the website.